|
READ
QUESTION AND ANSWERS PRESS SESSION WITH DOCTORS BELOW
The
World Health Organisation (WHO)
said today it is recommending new measures, related to international travel,
aimed at reducing the risk of further international spread of severe acute
respiratory syndrome (SARS).
The recommended measures include screening of air passengers departing
from a small number of affected areas on flights to another countries. The
affected areas, where transmission of the SARS infectious agent is known to
be spreading in a human-to-human chain, are kept under constant review and posted each day on the
WHO web site. At present, only four countries
are concerned - Canada (Toronto), Singapore, China (Beijing, Guangdong, Hong Kong,
Shanxi, Taiwan), Vietnam (Hanoi).
WHO
has said that no additional precautions for the screening of departing passengers at airports in any other parts of the world are called for in
these recommendations.
The screening measures, recommended for consideration by national health
officials and port authorities, involve an interview with passengers, departing from a limited number of areas, to detect illness with symptoms
that give reason to suspect that a passenger may be infected with SARS.
National authorities may wish to advise travellers with fever, departing on
international flights from the few areas where SARS transmission has been
documented, to postpone travel until they feel better. All international
travellers should be aware of the symptoms of SARS and seek immediate medical attention should symptoms occur.
Since global surveillance of SARS began at the end of February, some
evidence suggests that a small number of suspected and probable cases of
SARS have departed from the small number of affected countries on flights
to other countries.
Most cases continue to occur in persons in close face-to-face contact with
SARS patients. Close face-to-face contact could conceivably occur in an aircraft among persons seated close to a person infected with SARS and
coughing or sneezing.
WHO has also issued detailed recommendations to airlines on steps to take
should a suspected case of SARS be detected in flight. The WHO recommendations include advice on step-by-step procedures for following
up fellow passengers on the flight who may have had close contact with the
possible case and the specific advice that should be given to these travellers and their families.
The
WHO said that many national health authorities have
already issued their own SARS-related advice to international travellers.
=====
QUESTIONS
AND ANSWERS
The
situation regarding SARS is causing the travel industry within Asia and
in other parts of the world perhaps more damage than the war in Iraq,
but as with the war, the situation regarding SARS, precautions taken etc
are a little confused.
For
this reason we have below the complete Questions and Answers session
from a press conference with Dr Mark Salter, coordinator of the SARS clinical management collaborative network, Dr David Heymann, Executive Director of Communicable diseases, Dr Klaus Stohr, coordinator for the collaborative network of SARS research laboratories, and Dr Max Hardiman, Project Leader for International Health Regulations.
The press conference took place at the Palais des Nations, 27 March
2003.
As
many of the questions and answers are travel related we felt it may help
to clear up some of the confusion.
START
Q.
In stepping up travel recommendations, can you be a little more specific.
Is WHO now issuing travel guidelines that people from the affected areas
should go through some screening before they can get on board the aircraft? Who will do this? Is it the local authorities? Are there any guidelines
for people going to the affected regions?
A. Dr Max
Hardiman: Yes, it's a very simple screening procedure that we are
recommending. It's a matter of answering two questions about possible symptoms that a person might have of SARS and about contacts with
possible SARS cases. Those questions can be carried out in the same way as the security checks are carried out currently at check-in. Of course the
people doing that kind of work are not health trained, so if there is any doubt
about whether the person is positive, answering that they have symptoms or
that they have been in contact, then they can be referred to a health care
worker. This is going to be a difficult thing for the authorities to manage
because they will need extra health staff at airports. But this is important to
reassure the rest of the world that everything is being done to prevent the
spread of this disease further afield.
In response to your second question, we are not recommending any
restrictions to travel to any destinations. That recommendation still holds.
Dr
Heymann: Let me just add to what Max said. Countries still have the
option of making their own recommendations. We make a global recommendation for international spread, but countries may find that
because of other situations than just the epidemiology that it is necessary to
advise their citizens that travel should not be done. This would fall within the
scope of what we have provided, and we understand that countries may do this for a variety of reasons, including the fact that they may not be able to
have insurance to cover their workers in those countries so they want their
workers not to be at risk, or what the insurance companies feel is a risk. So
we have allowed countries to make their own recommendations.
Q.
Two questions if I may. First of all you say now, Dr Heymann, that the
Chinese are cooperating but I've seen various newspaper stories that say
they have been extremely lax in the beginning, at the end of last year when
this was spreading in the Guangdong region. And apparently still today the
provincial authorities are quite helpful but the Ministry of Health in Beijing is
still dragging its feet in making these statistics known, as indeed they seem
to have done in the cases of the early onset of AIDS in China. Now why are
they doing that? Is there any political reason, are viruses in any way connected with socialism or communism or something?
A. Dr David
Heymann: Well I think we all know that infectious diseases know
no borders and they respect no borders. Our understanding is a bit different.
Our understanding is that there has been full collaboration with the Ministry
of Health, that decisions are presently being made above the Ministry of
Health and these include discussions with decentralized provinces, which in
certain instances over health have more authority than central government.
So we understand it a little bit differently and this is a very complicated
negotiation that is going on between the various groups concerned, but we
are very optimistic that information has now got to the very high levels of
government and that there is attention being paid to these issues.
Q.
The second question. You said in the beginning that a close contact is
really the only danger of infection. You said when we were sitting in this
room that nobody would be at risk unless we are sitting next to you. But
apparently travelling in an airplane where ventilation is not optimal anyway
is now also considered a heightened risk. Is that correct? Your colleague
said that pilots have been given instructions if somebody gets ill on the
plane to take action. We would like to know what kind of action. Are they
being isolated?
A Dr Max Hardiman:
The kinds of contact that have resulted in transmission
of this disease I think you've probably heard about before: heath care workers and then in their families. We say close contact. Now close contact
can take place in a number of situations, including on aircraft, and we have
always been aware that there is the possibility that such contact could take
place in an aircraft or in any situation where you are very close to other
people. We had no evidence to suggest that it was happening in aircraft until
a recent case in Hong Kong, which you probably are also aware of, which seems to be linked to a probable case on an aircraft, which infected others.
We have defined what we mean by a close contact within the aircraft situation in the guidance that we are sending out. This is based on the best evidence that we have at this moment. As we learn more about the disease we may change that. But in fact we still think close contact is the important factor and it's not that the whole of the aircraft is going to be at risk, but those who are close to the person who is sick on the aircraft. That person can then be isolated, they can wear a mask, and that will cut down any risk of exposure enormously. But the other thing important to remember is that on an aircraft you don't usually have someone who is capable of making a decision, "this person is a case of SARS" or not. So what you are generally dealing with is someone who becomes sick on an aircraft and causes concern, and in order to reassure the passengers that they are getting the least opportunity for exposure possible that person can be isolated from other passengers and crew, can wear a mask, and can then be assessed when they arrive at their destination to see whether there is a possibility that this is SARS or not and the appropriate follow-up steps for any close contacts.
Q.
What is close contact aboard an
airplane? Sitting next to a passenger?
A. Dr Max
Hardimann: Sitting next to a passenger, sitting in the same row, or
sitting two rows in front or two rows behind. Also the stewardesses or flight
attendants would also be included as close contacts. Dr David Heymann. I
might also add that there has been great concern expressed by you about community spread. As I have said, as we have all said in the past, to date
there have been no cases which couldn't be linked in a chain of transmission from one person to another. Now as the epidemic continues to
go on, we are hearing that it is more and more difficult to find those source
patients in the next succeeding generations of cases. That is why it is very
important now for us to have the Guangdong information, which is four months' worth of information, which will help us understand if in
Guangdong there were cases which could not be traced back to another case. But in areas where there are many many cases, such as Hong Kong, it
is becoming more and more of a job to do all the investigations and to clearly link at this point all the cases with another case. But that is not to say
that there is not a link. It is only to say that as the epidemic increases in
numbers it is more difficult to trace those contacts.
Q.
Are you issuing a list of countries that should undertake this screening, or
if there isn't a list is there a case limit, or what is the definition?
A. Dr Max
Hardiman: We have on the WHO SARS Web site a list of what we
have called "affected countries". These are really countries where we have
evidence that there is transmission of the disease as opposed to maybe one
or two or three imported cases, which do not transmit any further. Those
affected countries are listed there and those are the ones where we suggest
this screening be applied. The countries are Hanoi, Vietnam; Singapore;
Hong Kong; Taiwan, China; Guangdong province, China; Toronto, Canada.
Q.
The two basic questions that will be required to be asked at airports
before people board, do we know what these two questions are? Do you have a sample? Secondly, what about people travelling by sea, passenger
liners and commercial cargo shipping?
A. Dr Max
Hardiman: The main concerns have been related to air transport,
but we have made the same recommendations for people travelling by sea, road or rail. The questions are basically, one question relates to symptoms,
asking about fever, cough or difficult in breathing. The second question
asks about possible exposures, whether you know you have been in contact with a case of SARS, whether you have worked or visited or been a
patient in a hospital where there is SARS, or whether you have member of
your family has been a suspect or probable case of SARS.
Q.
We heard earlier that you were not working with Taiwan. Can you
comment on this?
A. Dr David
Heymann: I don't think that you have heard that we are not
working with Taiwan. There is a WHO collaborating centre, which has actually had an expert working with the Taiwanese government since report
first came to WHO. So we receive reports of SARS probable cases. We contacted one of our partners, a collaborating centre that has had an expert
working with the Taiwanese government, and we have also posted on our Web site the cases that have been reported from Taiwan.
Q.
Regarding the travel advisory, do you have any plan to speed up the
safeguarding measures on the general situation, because some school in Singapore has already been shut down?
A. Dr Max
Hardiman: I'm not sure I understand your question. We are not
suggesting that countries be shut down. In fact we are suggesting that countries step up the measures that they are taking to ensure that flights
leaving their countries will not have passengers with SARS on in order to
prevent unnecessary disruption to travel.
Q.
Some country has already advised their citizens against travelling to the
affected areas. Do you encourage such kinds of moves?
A. Dr Max
Hardiman: Right, I understand your question. As David Heymann
said earlier, we recognize that individual countries have the right to make
their own advice for their own particular nationals. Sometimes they have to
take into account factors that we, in giving our recommendations, do not
have to take into account, such as these insurance issues and whether you
can medivac people out of that area. Those reasons can sometimes lead them to a different decision to WHO advice.
Q.
On the virus that is causing SARS, are you still thinking that it might be
the combination of the corona virus and the PM virus?
A. Dr Klaus
Stohr: We believe that the corona virus is the major causative
agent. Now the data that is forthcoming from very many different laboratories which investigated samples from Viet Nam, from Hong Kong,
from Singapore, from Germany, and from Canada, all these laboratories are
consistently finding corona virus in those patients. At the same time, the
laboratory in Hong Kong as well as CDC have isolated a virus from patients
and they could characterize this virus as a corona virus and they could also
develop certain tests, and they find that this test is positive in SARS patients
and that the test is negative in other healthy adults. This testing now allows
in the very near future to differentiate between those people who are affected and those who are not affected. This testing will start tomorrow in
Hong Kong. Hong Kong University has developed two different tests: one test looks into the blood of infected patients and sees if there are any
antibodies; the other test can detect virus in the respiratory tract, for
instance in saliva. These two tests in combination will allow to detect SARS
patients at an early stage. These are the very good preliminary results. We
need to take into account that these tests have not been validated, but this
starts tomorrow. The development of these tests is the result of a collaborative effort of all the laboratories that are members of this network.
Two outstanding breakthroughs or detections were made by two
laboratories and that is the Hong Kong University as well as the Centers for
Disease Control in Atlanta, USA. All of them are working in our WHO network.
Q.
So the paramyxo virus was not the cause of this disease?
A. Dr Klaus
Stohr: There are normally few diseases which are cause by two
pathogens. The majority of diseases are caused by only one pathogen. Now
we are seeing here consistent isolation of one pathogen in very many SARS
patients. That gives us confidence that corona virus is linked to SARS. What
we are also seeing is that some of these patients have another virus, a paramyxo virus. We have to find out what the second virus is doing. It could
potentiate the disease, that�s one possibility. It could be a helper virus which
enables the other virus to cause the damage or it could also be a co-infection and not related whatsoever with
SARS.
Q.
On the figures of China, Dr Heymann, you mentioned for Beijing and
Shanghai we have figures up to yesterday, 26 of March. Did you have information from Guangdong? What are the difficulties? They have been
reviewing what are the number of cases from March onwards. Why do they not have it?
A. Dr David
Heymann: I can�t answer that question. All I can say is that we�ve
been told that we will have that information very shortly. I think what�s going
on is that since there is a case definition internationally that describes the
disease, they�re making sure that what they report, recent reports, fit with
that case definition. And although their case definition was very close to
what we use in WHO world wide, there were some slight differences. So I think they�re just being doubly sure now on these cases that they have
counted since the beginning of March, to make sure that they fit the WHO
case definition. That�s what our understanding is from talking with the team.
Q.
Also a follow-up on that. Dr Salter, you mentioned that the two groups of
patients, 90% they got well 6 or 7 days afterwards, while 10% deteriorated.
So I wonder what are the characteristics of the group of patients that actually turned worse? Because they are some press reports suggesting it
has to do with age? Like someone over 40 or something. And do you also have the recovery rate of the disease?
A. Dr Mark Salter: I can start perhaps with the discrimination to the groups.
There are approximately, 90% of the individuals seem to be recovering when
they reach 6 or 7 days. We are not yet in a position to say that they are cured
but we having a number of reports of individuals being discharged into the
community who are apparently well but that�s obviously something that we
will need to follow up on. As for the 10% that are progressing to the more
severe form, the only prognostic indicators we have are for poor prognosis,
is that there seems to be a greater number of older people, and unfortunately
the figure 40 came out, although obviously most of us here would not consider that old. And that those individuals who progress to the more
severe group had previous existing illnesses before they developed SARS.
For example, they might have coronary heart disease or they might have renal impairment, kidney impairment, or they might have liver dysfunction.
Q.
The 40, so it is the dividing line or what?
A. Dr Mark Salter: It�s not a dividing line. We haven�t had sufficient statistics
to put an absolute figure on, but speaking to the clinicians yesterday, this is
the age above which they have seen most deaths.
Dr David
Heymann: And remember that the initial outbreaks are in hospital
workers who have this age. What we don�t have is the full range of ages yet,
hopefully we won�t have that, but the full range of ages that get sick.
Because there may be a different analysis in two weeks.
Q.
For Dr Heymann, a question from a lay man. Where do we stand on the,
you know, you said that there are several hundreds of cases, now perhaps
over a thousand, and it becomes harder and harder to track the contacts, as
they proliferate. Can you give us a sort of prognosis about the shape of
things to come? Is this going to be a pandemic after all or can it be stamped
out? And another thing, you talk about corona virus but this is then a new
variety of corona virus or is this already a well known one?
A. Dr David Heymann: I�ll speak to the pandemic question. In countries
where they�ve applied stringent measures and encouraged participation of
the international community, for example, in Viet Nam, the outbreak has been stopped, we believe that cases have not increased in the last three or
four days and we are hopeful that that outbreak is now contained and will
not continue. But we�re not sure yet. What you have to do is wait for two full
incubation periods after the last case of disease in order to declare that there
is no more transmission. In Singapore, measures are underway, very severe measures in some instances with quarantine which is justifiable in
the Singapore situation, and they seem to be confident that they are stopping the transmission. Hong Kong has increased recently its control
measures dramatically. But the difficulty in Hong Kong is that because they
are so many health workers infected, who are the pillars of the health care
system, it�s very difficult now to find all the extra health workers they need to
increase their measures. But our word from Hong Kong today was that they�re very confident now and that they�re increasing some of their
measures. Over the next 24 hours, they will be announcing this and they believe that it�s contained in Hong Kong. In Canada. there has been some
transmission to health workers and they�re now containing that outbreak
and we believe that�s been contained. The unknown, of course, is, number
one, is there an asymptomatic form of this disease, which means people are
infected without symptoms, who have been travelling around the world with
this disease. We don�t know that yet. We don�t believe that�s the case, we
hope that�s not the case. So the answer to your question of �will this
become a pandemic?�, we don�t believe it will become a pandemic, especially because after the alert that we raised, there�s been a heightened
search for cases in most countries and cases have been isolated immediately and stopped. So we think that the measures that we�ve have
sensitized the world and are preventing a disease from becoming a major pandemic. And that�s our hope.
Dr Klaus Stohr: The question was, is this a new virus which has been
detected. Now, three laboratories are looking at the genetic material of this
virus and the data that we have so far, clearly indicate that this is a new
strain which is unlike any known animal or human corona virus. In the corona virus group you have quite a few very aggressive animal viruses.
You have also viruses cause mild respiratory disease, you have viruses which cause diarrhoea. In humans, you have corona viruses which cause
coughing, sneezing, also those which cause pneumonia. However, this virus is none of the known viruses. That�s what the genetic analysis shows.
What is important here is that, I mean, this is scientifically important to know to which family this virus belongs. What is more important now for control, is to develop tests to differentiate infected from non-infected persons; tests which would help identify a person who might excrete the virus, who may not excrete the virus. This could be a major breakthrough in containment of the disease. Therefore, a lot of time is being invested by the laboratories to develop this est. That will then help also define what is a suspect, a probably, perhaps a confirmed case, that will also then speed up certainly measures to contort the disease. The emphasis is on diagnostic tests. Of course, scientifically, it�s important to understand what type of virus we have, to which sub-group it belongs. But we need a test to differentiate between healthy and infected patients.
Q. What does the discovery of the virus mean in terms of finding a treatment
then? I mean, is this going to, how quickly can this follow on, treatment or a
vaccination?
A. Dr Klaus Stohr: That�s at a very early stage. We must not forget that on the 17th of March which is last, I think Monday last week, a group of laboratories started looking at the etiology and now ten days later, the virus is more or less identified. The next step will be a diagnostic test. And I think all of the resources will be focusing on the diagnostic test. Now, understanding the genetic composition of the virus will then immediately lead to deliberations about the development about specific intervention measures and the first one, as you say, is a vaccine. But again, we are 10 days in the race for the virus and we have found a major suspect already. That�s not too bad. The other specific intervention would be a drug and I�m no sure if anyone has had time to think about it. But Mark might have an idea.
Dr Mark Salter:
As Klaus said, it�s very early days and in terms of actually addressing the issue in terms of the clinical pattern that we�re in patients, what is more important is that we come to understand the disease and how the host, the patient, is reacting to that organism, if it indeed is this virus. What the clinicians are doing, are working through standard therapeutic approaches which they would normally imply if patients were presenting with the disease that they wouldn�t initially know the cause of. So a number of well-described therapeutic regimes using various antibiotics have been
tried. Unfortunately, the results to date suggest that none of them have been effective in actually reducing the progress of those who would progress anyway. The drug ribavirin, an antiviral agent, has come into the frame by lots of people now, both media and clinicians, those who have actually been treating SARS patients and those of who haven�t. Ribavirin is an antiviral agent which has been proven to be effective in treating some of the paramyxo viruses like respiratory synctial virus in young children or in treating some of the more severe forms of viral haemorrhagic fever such as Lassa. However, it�s use in the treatment with SARS has been unremarkable to date. And it is hoped that now we have a large group of clinicians working together with WHO in this collaborative network, that we�ll be more readily able to assess the information from all patients that are given these therapies and hopefully come and establish what therapies are actually effective and rule out those therapies which have been proven to be ineffective, so that the clinicians can concentrate their efforts on looking at perhaps more novel approaches to aiding those who are suffering from the more severe form of
SARS.
Q.
Just, I wanted to clarify. Then, in fact identifying the virus doesn�t really help you in determining a treatment then, these are totally separate scientific processes?
A. Dr Mark Salter: At the present moment in time, they run in parallel, as all of these things do and at any one stage in any new disease, we are looking at all these things in one go. I think some people have the impression that we are looking at the virus isolation identity in isolation from the management of the patients, which isn�t the case. They are being looked at in parallel and the groups are working closely together. Once we actually can have a handle on the virus, there is the opportunity, as Klaus was saying, to start looking at experiments in tissue cultures to see what effectiveness therapies might have on blocking the replication of that virus in those tissue cultures. But that is only the firs stepping stone to actually developing and understanding what effective therapies there may be already in existence, or what effective therapies there may be yet to come.
Dr Klaus Stohr: The most important condition to develop a vaccine is to have the virus isolated in pure culture, either in animals or in cell culture. Then you can produce large amounts of this virus, inactivate its aggressivity, its pathogenicity for humans and test whether it causes any immune reaction in animals or people. So the condition for the development of the vaccine is the isolation of the virus. And that took place already on the 21st of March. And the first one who isolated the virus was Hong Kong University. And that was repeated and confirmed and (garble) had not been possible with the other network members, for instance, Centers for Disease Control in Atlanta. So the stepping stones are there for a vaccine but not much research has started on it.
Q.
I�ve got a follow-up question to your answer earlier. Aside of the vaccine or whatever to combat the SARS, from the history of the patients that are recovering, why are they recovering, besides being on machines? Shouldn�t that be giving you an indication why some people are getting better? What are the case histories showing?
A- Dr Klaus Stohr: What�s very promising is that patients who survive SARS have antibodies in their blood and these antibodies in cell cultures, outside the patient, can kill the virus. So that shows that these antibodies play also a role, potentially, of killing the virus in the body of the patient. So which means that this virus could also be used to immunize others before they are being infected, so that they would develop these antibodies before they are being infected by the real virus. But this is very promising. What keeps people alive, actually, is what Dr Heymann kept on saying during the last week, is supportive treatment. And those patients who have the immunity to develop antibodies, they can clear the virus from their body and they will then recuperate.
Q.
I want to go back to the question of close contact, because in the situation in Hong Kong, we have several hundred infected people already and for us mostly we have skyscrapers and high buildings. So going out or coming home, that means taking a lift, a escalator and I suppose that would be close contact for people to spread the
disease. Do you have any recommendation on that?
A. Dr David Heymann: The best prevention for any disease is information and understanding by people what that disease looks like and what they should do if they become sick. With that information, people can decide whether or not they want to expose themselves to what they consider at risk. It may be, for example, that somebody is coughing on an airplane
and the person next to them feels that they need to move in that airplane because they are afraid that this might be SARS. That�s a personal decision. And so, public health can�t do a lot for a disease which is a contact diseases, it has to be individuals who understand what the disease is. If somebody�s coughing, somebody looks like they are sick, the best would be for the person to be avoided by others. So that if you�re standing next to someone on a escalator who�s coughing , you ought to move back two or three steps. So that it�s a personal understanding of the disease that�s very important. It stops panic, it stops inappropriate measures, it stops trying and protect and giving yourself false security that you are being protected by something which won�t protect. So, what you people do is very important because that educates the general population as to what this disease is and how individually they can prevent themselves from beginning sick. So it�s an educational effort.
Q.
So just to follow up in that case. When you talk about close contact, what exactly kind of contact are we talking, spittle? Are we talking sneezing? Are we talking shaking hands, perspiration, touching an elevator button after someone else has touched it, who is infected? Secondly, could you just remind me, I�m sure you�ve said this before, what the incubation period is? And there are numbers on, have any children been infected with
SARS?
A. Dr David Heymann: The incubation period is 3-10 days as far as we understand, although information coming from Guangdong may provide more information that this is a little bit longer than 10 days. But right now we say a range of 3-10 days. Children are becoming ill, children of hospital workers who have become sick and many of these have been in school and people who are sitting by them are now also at risk. The disease. we believe, is spread by droplets but droplets which aren�t aerosolized and spreading a long way away. What I�ve always said is that in this room, the two people on each side of me would, from what we understand, be at more risk than you sitting there because this disease can spread through the air on heavy droplets and infect my next door neighbour but probably doesn�t go in finer droplets which are aerosolized which would eventually reach you. Measles, if I had measles, and you did not have measles, you could very well get measles because that would be a fine aerosol which would make it all the way to you. So this is limited to two seats in front, two seats in back of an
airplane, we believe, close contact, standing next to someone on an escalator who coughs on you, or other issues where you are in close contact, face to face, or very close. We don�t know about perspiration, but we don�t think so.
Q.
Are we certain now that this originated in Guangdong, that that is the real first focus of it and, second, is this corona virus we are talking about a virus which jumped the species barrier?
A. Dr David Heymann: The origin is really not important. It�s with us today and we have to stop it. As you look back, you�ll probably find that cases are traced back in generations and probably Guangdong will play a major role. Whether it�s the source of this outbreak, nobody can say. New viruses usually don�t come in from outer space. They come in from another organisms those viruses or bacteria, in this case virus�s. That could be animals, it could be another person who has a virus that mutates and is transforming that virus. But it�s usually which is already infecting something in nature, which either mutates or crosses this species barrier. Klaus, do you want to add anything more.
Dr Klaus Stohr: Many corona viruses of humans can be found in animals, particularly in mice. There have been tests run in China as well as in Canada and people found antibodies with traces of human corona virus in mice and also in bovines. So what are seeing is that these viruses appear to be transmissible in a way that they cause some antibody reaction but many not cause disease. These viruses change, everything changes, particularly viruses, and with the change of the virus, they might acquire new characteristics. And one of the characteristics could be species specificity, like influent viruses, they also can jump the species barrier. So that�s one of the possible explanations and research will help where these viruses are coming from. And that will also help us for the future, perhaps to anticipate the emergence of these viruses, so research is vitally important to understand where the virus comes from to see if something new might be happening in the future.
Q.
About the planes again, am I too mean to think that people might lie?
A. Dr Max Hardiman: You�re quite right, of course, people can lie and that�s why this won�t be a 100% and will not prevent 100% of people who are infected from getting on aeroplanes, but it will prevent those who doing so unknowingly, because they will be questioned before hand and made to realize that they should not take the flight. Also when there is a concern, from what we know of this disease, the infections are spread when people are ill not when they�re well, once they�ve been infected. So if someone looks very ill, they could also be referred to a health care worker, even if they�ve said they haven�t had any contact or had a cough. So, we can�t be a 100% but it will help to reduce, it�s the maximum we can do to prevent people from boarding planes.
Q.
What about the precautionary principle? Should all passengers on international flights wear a
mask?
A. Dr Max Hardiman: No, we don�t think would be helpful at all. Why? Because, one. it�s not very feasible, two, it would alarm people to a great extent, beyond what is reasonable for the danger associated with this disease and if people who are spreading the disease are sick, once they are identified them wearing a mask will be more effective than other people wearing masks for some of the time, not when they are eating their meal and so forth.
Q.
To go back to the escalator question because we do need your expert advice on that. When you mention close contact in the aeroplane, you said in the same row or two rows in front and two rows behind. So in escalator the size would be a little bit smaller than what you just describe. So if someone�s coughing in the lift I�m with, even if I try to do what Dr Heymann suggested, try to step back, it seems to me that there�s no escape. So would you recommend people to use a mask whenever they get into an escalator or something like that? Because it is a real issue for people in Hong Kong � we do it every day whenever we get out of our place and get home.
A. Dr David Heymann: Fortunately, from what we know about this disease, it seems that people who transmit the disease most are those who are quite sick, who have a fever, who are coughing. Fortunately, these people don�t often go far away from their homes and they go to health workers often. So again, I say that education is important and people who have cough and fever have just as much responsibility to go to a health worker as do people who are standing near them to protect themselves. So, it�s education, education, education, information, information, information. If everyone understands that this is a disease, and everyone
works together, it can be stopped no matter how close people have to be and I know they have to be very close in lifts and on escalators in Hong Kong. Max?
Dr Max Hardiman: Just to say that in all these exposures, there is no complete cut off - one is a completely safe thing to do and one is a completely unsafe thing to do. Sitting on an aeroplane for a transatlantic flight, you�re there for a lot longer and so your period of exposure could be much greater and therefore a slightly further distance might actually be taken into account.
Q.
So could you confirm that, there�s a news report that there will be an international conference on the SARS next week in Hong Kong?
A. Dr David Heymann: That conference, for many reasons, has been cancelled. Hong Kong has begun to cancel other events as well, as you know, concerts have been cancelled in Hong Kong. This is responsible public health. The Hong Kong authorities are attempting to minimize the possibility that people could be exposed to sick people in concert halls in other areas. So that meeting has been cancelled; it doesn�t happen to be because of Hong Kong cancelling it, it�s because it�s felt that we are getting enough information right
now on our telephone calls and it would not be of any added value to get everybody together. But that meeting will occur in the next three for four weeks, we believe.
Q. Will you change the venue?
A. Dr David Heymann: No, not that we know of.
END |

 Mandarin Oriental Opens Special Hotel in Beijing, China
Mandarin Oriental Opens Special Hotel in Beijing, China AirAsia to Launch Penang - Shenzhen and Kota Kinabalu - Shantou Flights
AirAsia to Launch Penang - Shenzhen and Kota Kinabalu - Shantou Flights Boeing Forecasts Passenger and Cargo Needs of China's Aviation Industry
Boeing Forecasts Passenger and Cargo Needs of China's Aviation Industry Air Corsica Takes Delivery of ATR's 1,700th Turboprop Aircraft
Air Corsica Takes Delivery of ATR's 1,700th Turboprop Aircraft Minor Hotels to Open Anantara Resort Ubud Bali in October
Minor Hotels to Open Anantara Resort Ubud Bali in October Uruguayan Air Force to Add A-29 Super Tucano Aircraft to Fleet
Uruguayan Air Force to Add A-29 Super Tucano Aircraft to Fleet Air Astana to Increase Flights to Phuket, Thailand; Signs Codeshare Deal with JAL
Air Astana to Increase Flights to Phuket, Thailand; Signs Codeshare Deal with JAL Hong Kong Airlines to Resume Long-Haul Flights with Seasonal Gold Coast Service
Hong Kong Airlines to Resume Long-Haul Flights with Seasonal Gold Coast Service IHG Signs Two Hotels in Quang Binh, Vietnam
IHG Signs Two Hotels in Quang Binh, Vietnam Marriott Opens Moxy Hotel in Mumbai, India
Marriott Opens Moxy Hotel in Mumbai, India Torsten Richter Returns to Minor Hotels as AGM of Indonesia and Malaysia
Torsten Richter Returns to Minor Hotels as AGM of Indonesia and Malaysia Minor Set to Open World's Third NH Resort in Maldives
Minor Set to Open World's Third NH Resort in Maldives Asiana Airlines and Air Serbia Appoint APG as GSA
Asiana Airlines and Air Serbia Appoint APG as GSA IndiGo to Launch New Delhi - Vijayawada Flights
IndiGo to Launch New Delhi - Vijayawada Flights Hong Kong Airport Reports Strong Increases in Cargo and Passenger Traffic
Hong Kong Airport Reports Strong Increases in Cargo and Passenger Traffic Delta Begins Rollout of Free Wi-Fi on Long-Haul International Routes
Delta Begins Rollout of Free Wi-Fi on Long-Haul International Routes Thai AirAsia X to Resume Flights Between Bangkok and Sydney, Australia
Thai AirAsia X to Resume Flights Between Bangkok and Sydney, Australia Marriott Partners Sonder to Add Over 9,000 Rooms to Portfolio
Marriott Partners Sonder to Add Over 9,000 Rooms to Portfolio IHG Opens Hotel Indigo in Bandung, Indonesia
IHG Opens Hotel Indigo in Bandung, Indonesia IndiGo Enhances Operations with Aviobook, an Electronic Flight Folder from Thales
IndiGo Enhances Operations with Aviobook, an Electronic Flight Folder from Thales Boeing Invests in Wagner SAF Refinery in Brisbane, Australia
Boeing Invests in Wagner SAF Refinery in Brisbane, Australia Aeroflot to Resume Flights Between Yekaterinburg and Bangkok, Phuket and Goa
Aeroflot to Resume Flights Between Yekaterinburg and Bangkok, Phuket and Goa Air Astana Takes Delivery of 56th Aircraft; Confirms Plan to Launch Phu Quoc Flights
Air Astana Takes Delivery of 56th Aircraft; Confirms Plan to Launch Phu Quoc Flights Seibu Prince Rebrands Hotel in Singapore
Seibu Prince Rebrands Hotel in Singapore airBaltic Appoints APG as GSA in Egypt
airBaltic Appoints APG as GSA in Egypt Korean Air and Delta Air Lines Partner Habitat for Humanity to Make a Difference in Cheonan
Korean Air and Delta Air Lines Partner Habitat for Humanity to Make a Difference in Cheonan Air New Zealand, Garuda, Qantas and Singapore Airlines Begin UPR Trials on 38 Routes
Air New Zealand, Garuda, Qantas and Singapore Airlines Begin UPR Trials on 38 Routes Thai AirAsia Reports Q2 and H1 2024 Results; Confirms Full-Year Targets
Thai AirAsia Reports Q2 and H1 2024 Results; Confirms Full-Year Targets EL AL Israel Airlines Finalises Deal for 31 Aircraft
EL AL Israel Airlines Finalises Deal for 31 Aircraft Cebu Pacific to Launch Davao - Hong Kong and Iloilo - Singapore Flights
Cebu Pacific to Launch Davao - Hong Kong and Iloilo - Singapore Flights Poland to Become Largest Operator of Apache Combat Helicopters Outside of USA
Poland to Become Largest Operator of Apache Combat Helicopters Outside of USA Singha Estate Partners Ascott for Rebranding of Two Hotels in the United Kingdom
Singha Estate Partners Ascott for Rebranding of Two Hotels in the United Kingdom IndiGo to Launch Coimbatore - Singapore Flights; Increase Frequency of Select Services
IndiGo to Launch Coimbatore - Singapore Flights; Increase Frequency of Select Services Parveen Kumar Joins Grand Hyatt Jakarta as General Manager
Parveen Kumar Joins Grand Hyatt Jakarta as General Manager Azerai Appoints Jimmy Tran as Group Director of Sales & Marketing
Azerai Appoints Jimmy Tran as Group Director of Sales & Marketing South Korea to Strengthen Airborne Surveillance and Reconnaissance Capabilities
South Korea to Strengthen Airborne Surveillance and Reconnaissance Capabilities Virgin Australia to Replace Fokker 100s with Embraer E190-E2 Aircraft
Virgin Australia to Replace Fokker 100s with Embraer E190-E2 Aircraft Cross Adds Two Hotels in Bangkok, Thailand to Portfolio
Cross Adds Two Hotels in Bangkok, Thailand to Portfolio airBaltic Exercises Options on 10 Airbus A220-300 Aircraft
airBaltic Exercises Options on 10 Airbus A220-300 Aircraft Etihad to Increase Thailand Flights; Resume A380 Service to Singapore
Etihad to Increase Thailand Flights; Resume A380 Service to Singapore Dusit Signs Hotel and Condo on Rama 3 Road in Bangkok, Thailand
Dusit Signs Hotel and Condo on Rama 3 Road in Bangkok, Thailand Cape and Kantary Hotels to Expand Portfolio with Serviced Suites in Korat, Thailand
Cape and Kantary Hotels to Expand Portfolio with Serviced Suites in Korat, Thailand Thai Airways Reports Q2 and H1 2024 Results
Thai Airways Reports Q2 and H1 2024 Results China Airlines Extends Cargo Handling Contract with FCS
China Airlines Extends Cargo Handling Contract with FCS Goldfinch Becomes First Piloted Electric Aircraft to Fly at NASA's Langley Research Center
Goldfinch Becomes First Piloted Electric Aircraft to Fly at NASA's Langley Research Center Rosewood Signs Luxury 33-Suite Resort in Exuma, Bahamas
Rosewood Signs Luxury 33-Suite Resort in Exuma, Bahamas British Airways Expands Codeshare with Bangkok Airways
British Airways Expands Codeshare with Bangkok Airways Aeroflot Unveils Most Popular International Destinations in H1 2024
Aeroflot Unveils Most Popular International Destinations in H1 2024 Marriott Executive Apartments Open on Sukhumvit Soi 49 in Bangkok, Thailand
Marriott Executive Apartments Open on Sukhumvit Soi 49 in Bangkok, Thailand Uday Rao Appointed RVP and GM of Four Seasons Hotel Tokyo at Otemachi in Japan
Uday Rao Appointed RVP and GM of Four Seasons Hotel Tokyo at Otemachi in Japan CapitaLand Ascott Trust Secures OCBC 1.5°C Loan
CapitaLand Ascott Trust Secures OCBC 1.5°C Loan Sabre Hospitality Enhances SynXis Booking Engine with Trip Protection Services
Sabre Hospitality Enhances SynXis Booking Engine with Trip Protection Services Cathay Pacific Orders 30 Airbus A330-900 Aircraft
Cathay Pacific Orders 30 Airbus A330-900 Aircraft Haytham Said Appointed GM of Four Seasons Hotel Miami
Haytham Said Appointed GM of Four Seasons Hotel Miami Hong Kong Airport Launches World's First Smartphone Express Bag Drop Service
Hong Kong Airport Launches World's First Smartphone Express Bag Drop Service Marriott Signs W Hotel in Hangzhou, China
Marriott Signs W Hotel in Hangzhou, China IndiGo Selects Recaro's R2 and R5 Seats for New A321neo Aircraft
IndiGo Selects Recaro's R2 and R5 Seats for New A321neo Aircraft Scoot to Take Delivery of Jalan-Jalan and Travel Kaki E190-E2s in September and October
Scoot to Take Delivery of Jalan-Jalan and Travel Kaki E190-E2s in September and October Ali Mohammed Appointed Regional Vice President and GM of Four Seasons Resort Orlando
Ali Mohammed Appointed Regional Vice President and GM of Four Seasons Resort Orlando Marriott Opens Fourth Executive Apartments Property in Bangkok, Thailand
Marriott Opens Fourth Executive Apartments Property in Bangkok, Thailand AirAsia X to Resume Kuala Lumpur - Chongqing Flights
AirAsia X to Resume Kuala Lumpur - Chongqing Flights Norse Operates Non-Stop Charter Flight from Oslo to Darwin, Australia
Norse Operates Non-Stop Charter Flight from Oslo to Darwin, Australia Wyndham Reports Record H1 Growth in Asia Pacific
Wyndham Reports Record H1 Growth in Asia Pacific LOT Polish Airlines Takes Delivery of First Embraer E195-E2
LOT Polish Airlines Takes Delivery of First Embraer E195-E2 Vietnam Airlines Takes Delivery of Fifth Boeing 787-10 Aircraft
Vietnam Airlines Takes Delivery of Fifth Boeing 787-10 Aircraft Marriott Expands Executive Apartments Brand to Penang, Malaysia
Marriott Expands Executive Apartments Brand to Penang, Malaysia AirAsia Group Expands Fleet with Four Airbus A321neo Aircraft
AirAsia Group Expands Fleet with Four Airbus A321neo Aircraft IATA Reports Latest Airline Passenger Traffic Data
IATA Reports Latest Airline Passenger Traffic Data China Airlines Signs SAF-Related MOU with Morrison Express
China Airlines Signs SAF-Related MOU with Morrison Express Fairfield by Marriott Hotel Opens in Terengganu, Malaysia
Fairfield by Marriott Hotel Opens in Terengganu, Malaysia IATA Reports Latest Global Air Cargo Data
IATA Reports Latest Global Air Cargo Data Marriott Opens Fifth Autograph Collection Hotel in Japan
Marriott Opens Fifth Autograph Collection Hotel in Japan Matthew Smith to Succeed Monique Arnoux as CEO of Destination Asia
Matthew Smith to Succeed Monique Arnoux as CEO of Destination Asia American Airlines Renews Subscription to Prism
American Airlines Renews Subscription to Prism Shanghai Pudong Airport Installs 52 Kiosks and 14 Self-Service Bag Drops from SITA
Shanghai Pudong Airport Installs 52 Kiosks and 14 Self-Service Bag Drops from SITA Hong Kong Airport Handled 4.3 Million Passengers and 29,590 Flight Movements in June
Hong Kong Airport Handled 4.3 Million Passengers and 29,590 Flight Movements in June Croatia Airlines Takes Delivery of First Airbus A220
Croatia Airlines Takes Delivery of First Airbus A220 Ryanair to Implement Boeing's Jeppesen FliteDeck Pro 5.0 EFB
Ryanair to Implement Boeing's Jeppesen FliteDeck Pro 5.0 EFB Asia Pacific Airlines Carried 28.9 Million International Passengers in June
Asia Pacific Airlines Carried 28.9 Million International Passengers in June Singapore Changi Airport Reports Q2 2024 Traffic
Singapore Changi Airport Reports Q2 2024 Traffic Cat Wu Returns to Singapore as Executive Director of Revenue for Two Hotels
Cat Wu Returns to Singapore as Executive Director of Revenue for Two Hotels Langham Appoints Jack Xiao as Senior Vice President of Operations - China
Langham Appoints Jack Xiao as Senior Vice President of Operations - China NATO Selects Sikorsky X2 Rotorcraft for Integrated Platform Concept Study
NATO Selects Sikorsky X2 Rotorcraft for Integrated Platform Concept Study Malaysia Airlines Expands Retailing Strategy with NDC Content on Travelport
Malaysia Airlines Expands Retailing Strategy with NDC Content on Travelport Air Tahiti Orders Four ATR 72-600 Aircraft
Air Tahiti Orders Four ATR 72-600 Aircraft One Air to Expand Fleet with Third Boeing 747-400 Freighter
One Air to Expand Fleet with Third Boeing 747-400 Freighter FCM Travel Expands Cytric Distribution Agreement with Amadeus
FCM Travel Expands Cytric Distribution Agreement with Amadeus Cathay Pacific Expands 1 Ticket, 1 Tree Initiative to Include Cargo
Cathay Pacific Expands 1 Ticket, 1 Tree Initiative to Include Cargo Japan Airlines Confirms Order for 20 Airbus A350-900s and 11 A321neos
Japan Airlines Confirms Order for 20 Airbus A350-900s and 11 A321neos Embraer E190 Freighter Receives ANAC Type Certification
Embraer E190 Freighter Receives ANAC Type Certification Libya's Berniq Airways Orders Six A320neo Family Aircraft
Libya's Berniq Airways Orders Six A320neo Family Aircraft Qatar Airways Adds 20 Boeing 777-9s to Order Book
Qatar Airways Adds 20 Boeing 777-9s to Order Book Accor Signs Raffles Hotel in Tokyo, Japan
Accor Signs Raffles Hotel in Tokyo, Japan Thai AirAsia to Launch Bangkok - Hyderabad and Phuket - Siem Reap Flights
Thai AirAsia to Launch Bangkok - Hyderabad and Phuket - Siem Reap Flights Courtyard by Marriott Hotel Opens in Sapporo, Japan
Courtyard by Marriott Hotel Opens in Sapporo, Japan Qatar Airways Unveils Qsuite Next Gen at Farnborough Airshow 2024
Qatar Airways Unveils Qsuite Next Gen at Farnborough Airshow 2024 British Airways Increases Number of Funded Places in Speedbird Pilot Academy
British Airways Increases Number of Funded Places in Speedbird Pilot Academy Mandarin Oriental Signs Hotel and Residences in Bali, Indonesia
Mandarin Oriental Signs Hotel and Residences in Bali, Indonesia Minor Hotels Signs Dual-Branded Property in Yining, China
Minor Hotels Signs Dual-Branded Property in Yining, China Korean Air Takes Delivery of First Boeing 787-10 Dreamliner
Korean Air Takes Delivery of First Boeing 787-10 Dreamliner Two Senior Promotions at IHG Asia Pacific
Two Senior Promotions at IHG Asia Pacific Miss International Queen 2024 (MIQ 2024) - Interview with Alisa Phanthusak, MD, Tiffany's Show Pattaya, Thailand
Miss International Queen 2024 (MIQ 2024) - Interview with Alisa Phanthusak, MD, Tiffany's Show Pattaya, Thailand Airbus A321XLR Powered by CFM LEAP-1A Engines Receives EASA Type Certification
Airbus A321XLR Powered by CFM LEAP-1A Engines Receives EASA Type Certification New Dusit Thani Bangkok Hotel to Open 27 September 2024
New Dusit Thani Bangkok Hotel to Open 27 September 2024 CWT Upgrades Airfare Optimization Service with AI and Machine Learning
CWT Upgrades Airfare Optimization Service with AI and Machine Learning Small Luxury Hotels of the World Returns to India with MRS Group Partnership
Small Luxury Hotels of the World Returns to India with MRS Group Partnership SATS and SF Group Sign MOU to Expand Global Footprint
SATS and SF Group Sign MOU to Expand Global Footprint Thai AirAsia to Launch Don Mueang - Lampang Flights
Thai AirAsia to Launch Don Mueang - Lampang Flights Hong Kong Welcomed 3.13 Million Visitor Arrivals in June 2024
Hong Kong Welcomed 3.13 Million Visitor Arrivals in June 2024 China Airlines Launches Direct Flights Between Taipei and Seattle, USA
China Airlines Launches Direct Flights Between Taipei and Seattle, USA London Heathrow Airport Expands Partnership with SITA
London Heathrow Airport Expands Partnership with SITA bp Partners Audi Formula 1 Team
bp Partners Audi Formula 1 Team Qantas Launches Non-Stop Flights Between Perth and Paris, France
Qantas Launches Non-Stop Flights Between Perth and Paris, France Marriott Signs First Ritz-Carlton Reserve in UAE
Marriott Signs First Ritz-Carlton Reserve in UAE Vietnam Airlines to Launch Flights Between Hanoi and Phnom Penh, Cambodia
Vietnam Airlines to Launch Flights Between Hanoi and Phnom Penh, Cambodia Saudia and flyadeal Increase Flights to Abha; Group Reports Positive H1 Numbers
Saudia and flyadeal Increase Flights to Abha; Group Reports Positive H1 Numbers SITA Completes Legal and Regulatory Formalities for Materna IPS Acquisition
SITA Completes Legal and Regulatory Formalities for Materna IPS Acquisition Marriott Opens AC Hotel in Gunpo City, South Korea
Marriott Opens AC Hotel in Gunpo City, South Korea Air France-KLM Signs Codeshare and Interline Agreements with Scandinavian Airlines
Air France-KLM Signs Codeshare and Interline Agreements with Scandinavian Airlines IHG Signs Four Hotels in Spain
IHG Signs Four Hotels in Spain Entries Open for 2025 New Zealand Millennium Cup Regatta
Entries Open for 2025 New Zealand Millennium Cup Regatta American Airlines to Develop Aviation Maintenance Talent Pipeline with Tulsa Tech
American Airlines to Develop Aviation Maintenance Talent Pipeline with Tulsa Tech IHG Signs First Vignette Collection Hotel in Almaty, Kazakhstan
IHG Signs First Vignette Collection Hotel in Almaty, Kazakhstan Hahnair Partners German Formula 1 Driver, Nico Hülkenberg
Hahnair Partners German Formula 1 Driver, Nico Hülkenberg Travelport Enhances Platform with AI and ML-Powered Content Curation Layer
Travelport Enhances Platform with AI and ML-Powered Content Curation Layer Cotai Water Jet to Launch Macau Fireworks and Sightseeing Cruises
Cotai Water Jet to Launch Macau Fireworks and Sightseeing Cruises United Airlines Applies to Launch New Daily DCA - SFO Service
United Airlines Applies to Launch New Daily DCA - SFO Service Luminara, a Ritz-Carlton SuperYacht, to Cruise Asia Pacific in 2025-26
Luminara, a Ritz-Carlton SuperYacht, to Cruise Asia Pacific in 2025-26 Afrijet Appoints APG as GSA in South Africa
Afrijet Appoints APG as GSA in South Africa Euros 2024 a Record-Breaking Success for Hotels in Cologne, Germany
Euros 2024 a Record-Breaking Success for Hotels in Cologne, Germany Etihad Airways to Increase Flights to Boston, USA; Operate A350 on Toronto Service
Etihad Airways to Increase Flights to Boston, USA; Operate A350 on Toronto Service Saudi Arabia Orders Four A330 Multi Role Tanker Transport Aircraft from Airbus
Saudi Arabia Orders Four A330 Multi Role Tanker Transport Aircraft from Airbus Ascott Becomes Official Global Hotels Partner of Chelsea FC; Will Take Over Stadium Hotels
Ascott Becomes Official Global Hotels Partner of Chelsea FC; Will Take Over Stadium Hotels Indochina Kajima Gets Green Light for Construction of Mandarin Oriental Bai Nom in Vietnam
Indochina Kajima Gets Green Light for Construction of Mandarin Oriental Bai Nom in Vietnam Rahul Dangwal Joins Amora Riverwalk Melbourne; Rob Unson Joins Amora Brisbane
Rahul Dangwal Joins Amora Riverwalk Melbourne; Rob Unson Joins Amora Brisbane Air Canada Signs Deal for Eight Boeing 737-8 Aircraft
Air Canada Signs Deal for Eight Boeing 737-8 Aircraft Cebu Pacific Takes Delivery of 7th Aircraft of the Year
Cebu Pacific Takes Delivery of 7th Aircraft of the Year SITA Reports Record Results; Future of Air Travel - Podcast and Video Interview with Sumesh Patel, President of SITA Asia Pacific
SITA Reports Record Results; Future of Air Travel - Podcast and Video Interview with Sumesh Patel, President of SITA Asia Pacific Vietnam Airlines Takes Delivery of First Airbus A320neo
Vietnam Airlines Takes Delivery of First Airbus A320neo Marriott Opens 100th Sheraton Hotel in Greater China
Marriott Opens 100th Sheraton Hotel in Greater China Syahreza Ishwara Appointed GM of Anantara Koh Yao Yai Resort & Villas in Thailand
Syahreza Ishwara Appointed GM of Anantara Koh Yao Yai Resort & Villas in Thailand Tiong Nam Hospitality Adds Marina in Puteri Harbour, Malaysia to Portfolio
Tiong Nam Hospitality Adds Marina in Puteri Harbour, Malaysia to Portfolio Sabah Tourism Board Signs 5-Year Agreement with AirAsia
Sabah Tourism Board Signs 5-Year Agreement with AirAsia Turkish Airlines to Expand Cargo Fleet with Four Boeing 777 Freighters
Turkish Airlines to Expand Cargo Fleet with Four Boeing 777 Freighters Zurich Airport to Trial Security Solutions from Smiths Detection
Zurich Airport to Trial Security Solutions from Smiths Detection IATA Reports Global Air Cargo Data for May 2024
IATA Reports Global Air Cargo Data for May 2024 AirAsia Launches KL - Sihanoukville Flights; Confirms KL - Labuan Bajo Service
AirAsia Launches KL - Sihanoukville Flights; Confirms KL - Labuan Bajo Service Inaugural Tourism Seasonality Summit to Take Place at Routes World 2024 in Bahrain
Inaugural Tourism Seasonality Summit to Take Place at Routes World 2024 in Bahrain Hahnair Adds 10 Airlines to HR-169 Ticket Solution
Hahnair Adds 10 Airlines to HR-169 Ticket Solution WFS Opens Fifth Cargo Terminal at Adolfo Suarez Madrid-Barajas Airport in Spain
WFS Opens Fifth Cargo Terminal at Adolfo Suarez Madrid-Barajas Airport in Spain Four Senior Appointments at New Dusit Thani Bangkok Hotel
Four Senior Appointments at New Dusit Thani Bangkok Hotel Onyx Opens First Shama Hotel and Serviced Apartments in Malaysia
Onyx Opens First Shama Hotel and Serviced Apartments in Malaysia IHG Signs First Hotel in Kashmir
IHG Signs First Hotel in Kashmir World's Largest Aloft Hotel Appoints Tan Kim Seng as General Manager
World's Largest Aloft Hotel Appoints Tan Kim Seng as General Manager AirAsia X to Launch Flights Between Kuala Lumpur and Nairobi, Kenya
AirAsia X to Launch Flights Between Kuala Lumpur and Nairobi, Kenya Minor Signs Deal to Rebrand Peace Resort Samui as NH Collection Samui
Minor Signs Deal to Rebrand Peace Resort Samui as NH Collection Samui Thai Airways Resumes Flights to Milan and Oslo
Thai Airways Resumes Flights to Milan and Oslo Kylie Minogue to Perform at Mandarin Oriental Bodrum's 10th Anniversary Party
Kylie Minogue to Perform at Mandarin Oriental Bodrum's 10th Anniversary Party Eve Air Mobility Raises US$94 Million in New Equity Financing
Eve Air Mobility Raises US$94 Million in New Equity Financing Thai AirAsia Launches Suvarnabhumi - Hat Yai Flights
Thai AirAsia Launches Suvarnabhumi - Hat Yai Flights Jesper Larsen Returns to Vietnam as GM of InterContinental Halong Bay Resort and Residences
Jesper Larsen Returns to Vietnam as GM of InterContinental Halong Bay Resort and Residences Six Key Appointments at Ascott
Six Key Appointments at Ascott Finnair Completes Long-Haul Cabin Renewal
Finnair Completes Long-Haul Cabin Renewal AirAsia to Launch Flights Between Kuala Lumpur and Chiang Rai, Thailand
AirAsia to Launch Flights Between Kuala Lumpur and Chiang Rai, Thailand Thai Airways Expands Partnership with Amadeus
Thai Airways Expands Partnership with Amadeus Asia Pacific Airlines Carried 27.9 Million International Passengers in May
Asia Pacific Airlines Carried 27.9 Million International Passengers in May Korean Air Cargo Expands SAF Program with CEVA Logistics Partnership
Korean Air Cargo Expands SAF Program with CEVA Logistics Partnership IHG Signs First Holiday Inn Express Hotel in Egypt
IHG Signs First Holiday Inn Express Hotel in Egypt Ticket Booking Opens for World Travel Market 2024 in London
Ticket Booking Opens for World Travel Market 2024 in London Spotnana Enhances Service with Sabre's NDC Content
Spotnana Enhances Service with Sabre's NDC Content Codeshare Flights Between Kuwait and Thai Airways Take Off
Codeshare Flights Between Kuwait and Thai Airways Take Off Singapore Airlines Extends Cargo Handling Contracts with WFS
Singapore Airlines Extends Cargo Handling Contracts with WFS Courtyard by Marriott Hotel Opens Near Colva Beach in Goa, India
Courtyard by Marriott Hotel Opens Near Colva Beach in Goa, India Air Mauritius Joins AirAsia Move OTA
Air Mauritius Joins AirAsia Move OTA LOT Polish Airlines Appoints APG as Online GSA in Saudi Arabia
LOT Polish Airlines Appoints APG as Online GSA in Saudi Arabia Onyx Hospitality Expands Shama Hub Brand to Hangzhou and Hong Kong
Onyx Hospitality Expands Shama Hub Brand to Hangzhou and Hong Kong Minor to Take Over Management of Iconic Hotel in Bangkok, Thailand
Minor to Take Over Management of Iconic Hotel in Bangkok, Thailand Singapore Airlines to Launch Flights to Beijing Daxing; Increase Beijing Capital Service
Singapore Airlines to Launch Flights to Beijing Daxing; Increase Beijing Capital Service Marriott Opens Fourth Courtyard Hotel in Malaysia
Marriott Opens Fourth Courtyard Hotel in Malaysia Momentus Hospitality Appoints Chow Keng Hai as General Manager
Momentus Hospitality Appoints Chow Keng Hai as General Manager Helicopter Designed for French Special Forces Begins Flight Tests
Helicopter Designed for French Special Forces Begins Flight Tests Westin Resort Opens in Cam Ranh, Vietnam
Westin Resort Opens in Cam Ranh, Vietnam Google Wallet Compatibility Added to Vingcard's Digital Key Solution, Mobile Access
Google Wallet Compatibility Added to Vingcard's Digital Key Solution, Mobile Access Cross Signs New-Build Resort on Batam Island in Indonesia
Cross Signs New-Build Resort on Batam Island in Indonesia Korean Air Increasing Select Flights to China and Japan
Korean Air Increasing Select Flights to China and Japan Air Astana Donates Upcycled Aircraft Furniture to Almaty Airport
Air Astana Donates Upcycled Aircraft Furniture to Almaty Airport Jetstar Asia Resumes Flights Between Singapore and Clark, Philippines
Jetstar Asia Resumes Flights Between Singapore and Clark, Philippines Sabre Hospitality to Showcase SynXis Concierge.AI at HITEC 2024
Sabre Hospitality to Showcase SynXis Concierge.AI at HITEC 2024 St. Regis Resort Opens in Al Mouj, Oman
St. Regis Resort Opens in Al Mouj, Oman Percy Muncherji and Ron Cusiter Join Thailand's Centara Hotels and Resorts
Percy Muncherji and Ron Cusiter Join Thailand's Centara Hotels and Resorts Four Seasons Yachts Unveils Details of More Voyages Planned for 2026
Four Seasons Yachts Unveils Details of More Voyages Planned for 2026 Sabre to Upgrade Sun Siyam Resorts' Distribution and Retailing Strategy
Sabre to Upgrade Sun Siyam Resorts' Distribution and Retailing Strategy Positive Outlook as Asia Pacific Airlines Return to Profitability
Positive Outlook as Asia Pacific Airlines Return to Profitability SITA Reports Continued Reduction in Mishandled Baggage by Air Transport Industry
SITA Reports Continued Reduction in Mishandled Baggage by Air Transport Industry Scandinavian Airlines Launches Daily Flights Between Copenhagen and Atlanta, USA
Scandinavian Airlines Launches Daily Flights Between Copenhagen and Atlanta, USA Belgium Orders 17 Airbus H145M Helicopters
Belgium Orders 17 Airbus H145M Helicopters AirAsia Resumes Direct Flights Between Kuala Lumpur and Pattaya, Thailand
AirAsia Resumes Direct Flights Between Kuala Lumpur and Pattaya, Thailand Vietnam Airlines Launches Flights Between Saigon and Manila, Philippines
Vietnam Airlines Launches Flights Between Saigon and Manila, Philippines Korean Air Selects Air Incheon as Preferred Bidder for Asiana's Freighter Business
Korean Air Selects Air Incheon as Preferred Bidder for Asiana's Freighter Business Marriott to Significantly Expand Portfolio of Hotels in France
Marriott to Significantly Expand Portfolio of Hotels in France Avianca Resumes Eleven International Routes
Avianca Resumes Eleven International Routes IHG Signs First Kimpton Resort in Hawaii
IHG Signs First Kimpton Resort in Hawaii Laurence Neumann Joins Gran Melia Nha Trang as DOSM
Laurence Neumann Joins Gran Melia Nha Trang as DOSM Frasers Hospitality Expands Sabre Partnership with SynXis Retailing
Frasers Hospitality Expands Sabre Partnership with SynXis Retailing IHG Signs Holiday Inn Resort in Kufri, India
IHG Signs Holiday Inn Resort in Kufri, India Charles Szar Joins AeroTransCargo as President
Charles Szar Joins AeroTransCargo as President Saudi Arabia's Travel and Tourism Sector Continues to Break Records
Saudi Arabia's Travel and Tourism Sector Continues to Break Records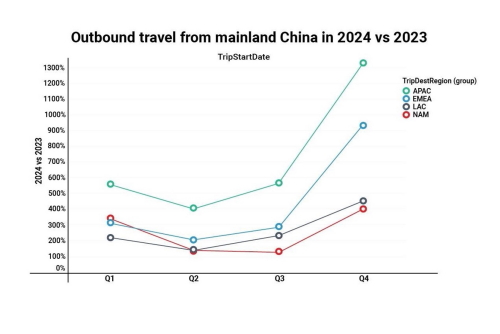 Sabre Market Intelligence Reveals Key Insights into China's Outbound Travel Trends
Sabre Market Intelligence Reveals Key Insights into China's Outbound Travel Trends Geoff Donaghy, CEO of ICC Sydney, Resigns
Geoff Donaghy, CEO of ICC Sydney, Resigns Emirates to Launch Dubai - Seychelles - Madagascar Flights
Emirates to Launch Dubai - Seychelles - Madagascar Flights Pan Pacific Returns to Jakarta with Tallest Luxury Hotel in the City
Pan Pacific Returns to Jakarta with Tallest Luxury Hotel in the City Saudia and Virgin Atlantic Sign Codeshare Agreement
Saudia and Virgin Atlantic Sign Codeshare Agreement SalamAir to Launch Flights Between Muscat and Delhi, India
SalamAir to Launch Flights Between Muscat and Delhi, India Radisson to Expand Red Hotel Brand to Bangkok, Thailand
Radisson to Expand Red Hotel Brand to Bangkok, Thailand Plaza Premium Expands Number of Personalised Services at Hong Kong Airport
Plaza Premium Expands Number of Personalised Services at Hong Kong Airport Vietnam Airlines Joins IATA CO2 Connect
Vietnam Airlines Joins IATA CO2 Connect Dusit Signs Dual-Branded Hotel and Residences in Phuket, Thailand
Dusit Signs Dual-Branded Hotel and Residences in Phuket, Thailand Hong Kong Airlines to Launch Flights to Da Nang, Vietnam
Hong Kong Airlines to Launch Flights to Da Nang, Vietnam Singapore University Working with SITA to Upgrade Air Travel Experience
Singapore University Working with SITA to Upgrade Air Travel Experience Germany Orders 38 Airbus H225 Helicopters for Bundespolizei
Germany Orders 38 Airbus H225 Helicopters for Bundespolizei AI to Reduce Food Waste at All Mandarin Oriental Hotels Globally
AI to Reduce Food Waste at All Mandarin Oriental Hotels Globally ITA Airways to Upgrade Network Infrastructure with SITA Connect Go
ITA Airways to Upgrade Network Infrastructure with SITA Connect Go Accor to Implement Amadeus' Cloud-Based Central Reservation System
Accor to Implement Amadeus' Cloud-Based Central Reservation System Gonzalo Aguilar to Join Minor Hotels as CEO - Europe & Americas
Gonzalo Aguilar to Join Minor Hotels as CEO - Europe & Americas Cathay Pacific and Singapore Airlines to Collaborate on Sustainable Initiatives
Cathay Pacific and Singapore Airlines to Collaborate on Sustainable Initiatives Minor Takes Over Management of Two Hotels in Sri Lanka
Minor Takes Over Management of Two Hotels in Sri Lanka CapitaLand Completes Acquisition of Standard at Columbia Student Accommodation in USA
CapitaLand Completes Acquisition of Standard at Columbia Student Accommodation in USA Singapore Airlines Renews Slot and Schedule Manager Agreement with Sabre
Singapore Airlines Renews Slot and Schedule Manager Agreement with Sabre Austrian Airlines to Increase Flights to Bangkok, Thailand
Austrian Airlines to Increase Flights to Bangkok, Thailand Riyadh Air and Singapore Airlines to Explore Interline Connectivity and More
Riyadh Air and Singapore Airlines to Explore Interline Connectivity and More Mandarin Oriental Opens Second Hotel in London, England
Mandarin Oriental Opens Second Hotel in London, England Mexicana Orders 20 Embraer E2 Aircraft
Mexicana Orders 20 Embraer E2 Aircraft Lufthansa Launches Flights Between Munich and Seattle, USA
Lufthansa Launches Flights Between Munich and Seattle, USA Airbus to Showcase Wingman Concept at ILA Berlin
Airbus to Showcase Wingman Concept at ILA Berlin Marriott Resort Opens in Lampung, Indonesia
Marriott Resort Opens in Lampung, Indonesia IndiGo and Japan Airlines Agree to Codeshare
IndiGo and Japan Airlines Agree to Codeshare Ritz-Carlton Reserve Opens on Ummahat Island in Saudi Arabia
Ritz-Carlton Reserve Opens on Ummahat Island in Saudi Arabia Norse Atlantic Airways Launches Flights Between Athens and New York, USA
Norse Atlantic Airways Launches Flights Between Athens and New York, USA British Airways Opens Refurbished Lounge at Lagos Airport in Nigeria
British Airways Opens Refurbished Lounge at Lagos Airport in Nigeria Hong Kong Airport Reports Robust Increases in Passenger and Cargo Traffic
Hong Kong Airport Reports Robust Increases in Passenger and Cargo Traffic Marriott Opens Luxury Collection Resort in Labuan Bajo, Indonesia
Marriott Opens Luxury Collection Resort in Labuan Bajo, Indonesia Dusit Expands Senior Development Team with Two Executive Appointments
Dusit Expands Senior Development Team with Two Executive Appointments Hong Kong Airlines to Launch Flights to Taichung, Taiwan
Hong Kong Airlines to Launch Flights to Taichung, Taiwan Aviation: RPK Up 11%, ASK Up 9.6 and PLF at 82.4% in April 2024
Aviation: RPK Up 11%, ASK Up 9.6 and PLF at 82.4% in April 2024 Furama to Rebrand Hotel in Sydney, Australia
Furama to Rebrand Hotel in Sydney, Australia IHG Signs Two Crowne Plaza Hotels in Egypt
IHG Signs Two Crowne Plaza Hotels in Egypt IATA Reports Latest Air Cargo Data
IATA Reports Latest Air Cargo Data Air Canada Expands Ottawa Network
Air Canada Expands Ottawa Network Marriott Signs Tribute Portfolio Hotels in Chongqing, Jiande and Xiaoshan, China
Marriott Signs Tribute Portfolio Hotels in Chongqing, Jiande and Xiaoshan, China Keishi Spa Swan Valley Relocates to Novotel Perth Murray Street in Australia
Keishi Spa Swan Valley Relocates to Novotel Perth Murray Street in Australia Korean Air's Afforestation Project in Baganuur, Mongolia Celebrates 20th Anniversary
Korean Air's Afforestation Project in Baganuur, Mongolia Celebrates 20th Anniversary Etihad Airways Becomes Main Sponsor of Girona FC
Etihad Airways Becomes Main Sponsor of Girona FC Rolls-Royce Adds Airline Support Baltic to Network of Authorised Service Centers
Rolls-Royce Adds Airline Support Baltic to Network of Authorised Service Centers Radisson Signs Blu Resort in Ho Tram, Vietnam
Radisson Signs Blu Resort in Ho Tram, Vietnam Treamprom Klinhom Joins Moxy Bangkok Ratchaprasong as MarCom Manager
Treamprom Klinhom Joins Moxy Bangkok Ratchaprasong as MarCom Manager The Slate Phuket Launches Promotion for Thai Residents
The Slate Phuket Launches Promotion for Thai Residents Airbus to Establish Tech Hub in Japan
Airbus to Establish Tech Hub in Japan Sabre Embraces Increasing Power of AI to Launch SabreMosaic
Sabre Embraces Increasing Power of AI to Launch SabreMosaic Thailand International Boat Show to Take Place at Phuket Yacht Haven in 2025
Thailand International Boat Show to Take Place at Phuket Yacht Haven in 2025 Aeroflot Opens Ticket Sales on Flights Between Krasnoyarsk and Sanya, China
Aeroflot Opens Ticket Sales on Flights Between Krasnoyarsk and Sanya, China Norwegian Cruise Line Unveils Details of 24 Port-Intensive Cruises Across Asia
Norwegian Cruise Line Unveils Details of 24 Port-Intensive Cruises Across Asia British Airways to Launch Seasonal Flights to Tromsø, Norway
British Airways to Launch Seasonal Flights to Tromsø, Norway SITA Expands Portfolio of Airport Solutions with Materna IPS Acquisition
SITA Expands Portfolio of Airport Solutions with Materna IPS Acquisition United Airlines Takes Wrexham AFC's Recent Success to New Heights
United Airlines Takes Wrexham AFC's Recent Success to New Heights Peter Tichy Joins Radisson Blu Plaza Bangkok as General Manager
Peter Tichy Joins Radisson Blu Plaza Bangkok as General Manager SMFL LCI Orders 14 Airbus Helicopters
SMFL LCI Orders 14 Airbus Helicopters Apollo Extends Charter Contract with Scandinavian Airlines (SAS)
Apollo Extends Charter Contract with Scandinavian Airlines (SAS) Garuda Indonesia and Singapore Airlines Sign FFP and Revenue Sharing Agreements
Garuda Indonesia and Singapore Airlines Sign FFP and Revenue Sharing Agreements Mandarin Oriental Signs Fifth Luxury Hotel in Italy
Mandarin Oriental Signs Fifth Luxury Hotel in Italy Saudia Signs Firm Order for 105 Airbus Aircraft
Saudia Signs Firm Order for 105 Airbus Aircraft IHG Signs Three Resorts in Turks & Caicos
IHG Signs Three Resorts in Turks & Caicos Plaza Premium Appoints Dr. Syafrina Sharif as Global Head of ESG & Sustainability
Plaza Premium Appoints Dr. Syafrina Sharif as Global Head of ESG & Sustainability TFE Hotels Launches New Loyalty Program
TFE Hotels Launches New Loyalty Program The First Collection at Jumeirah Village Circle Joins Marriott's Tribute Portfolio
The First Collection at Jumeirah Village Circle Joins Marriott's Tribute Portfolio Korean Air Partners AWS for AI-Powered Contact Center
Korean Air Partners AWS for AI-Powered Contact Center GOLIAT Project to Explore Use of Liquid Hydrogen in Aviation
GOLIAT Project to Explore Use of Liquid Hydrogen in Aviation Singapore Airlines to Establish a Foundation
Singapore Airlines to Establish a Foundation High-Speed Fun in Denmark! HD Video Interview with Aarhus Sea Rangers
High-Speed Fun in Denmark! HD Video Interview with Aarhus Sea Rangers 16 Exclusive HD Video Interviews from Routes Europe 2024 in Aarhus, Denmark
16 Exclusive HD Video Interviews from Routes Europe 2024 in Aarhus, Denmark 9 Exclusive HD Video Interviews from Routes Asia 2024 in Langkawi, Malaysia
9 Exclusive HD Video Interviews from Routes Asia 2024 in Langkawi, Malaysia 9 Exclusive Video Interviews with VIPs at ASEAN Tourism Forum 2024 in Vientiane, Laos
9 Exclusive Video Interviews with VIPs at ASEAN Tourism Forum 2024 in Vientiane, Laos 8 NTO Press Conferences from the ASEAN Tourism Forum 2024 in Vientiane, Laos
8 NTO Press Conferences from the ASEAN Tourism Forum 2024 in Vientiane, Laos 13 Exclusive HD Video Interviews with VIPs at World Travel Market 2023 in London, England
13 Exclusive HD Video Interviews with VIPs at World Travel Market 2023 in London, England 5 HD Video Interviews from APG World Connect 2023 in Monaco, France
5 HD Video Interviews from APG World Connect 2023 in Monaco, France 15 Exclusive Videos from Routes World 2023 in Istanbul, Türkiye
15 Exclusive Videos from Routes World 2023 in Istanbul, Türkiye
 - Interview with Alisa Phanthusak, MD, Tiffany's Show Pattaya, Thailand")

 Central Poland - Interview with Robert Makowski, Commercial Director (CCO)")

, Southampton (SOU) and Aberdeen Airports (ABZ) - Interview with Christopher Tibbett, Aviation Director")

 in Denmark - Interview with Lotta Sandsgaard, CEO, at Routes Europe 2024")



 - Interview with Prof. Dr. Martin Roll, CEO, at Routes Europe 2024")
 - Interview with Michiel Parent, Commercial Director")
 - Interview with Marc Watkins, RDM")
 in Estonia - Interview with Eero Pärgmäe Board Member and CCO")
 - Interview with Gary Cobb, Airport Director")





 in Western Australia - Interview with Stephanie Juszkiewicz, SVP Aviation Business Development, at Routes Asia 2024 in Langkawi, Malaysia")
 Rayong / Pattaya, Thailand - Interview with Ampika Chadawong, at Routes Asia 2024 in Langkawi, Malaysia")
 in Nha Trang, Vietnam - Interview with Le Thi Hong Minh at Routes Asia 2024 in Langkawi, Malaysia")



 - Interview with Simon Miller, Senior Manager Market Intelligence, at Routes Asia 2024 in Langkawi, Malaysia")













 at ATF 2024")






 2024 in Vientiane, Laos")





 to Rebrand as DTH Travel - HD Video Interview with Stephan Roemer, Partner and Group CEO")

 - HD Video Interview with Rohan A. Khaunte, Minister for Tourism at WTMLDN 2023")

 Tourism - Interview with Prateek Hira, President & CEO of Tornos, at WTMLDN 2023")

 - Interview with Sheo Shekhar Shukla, Principal Secretary Culture & Tourism, at WTMLDN 2023")
 - Interview with Dr. Rashmi Sharma, Director - Department of Tourism, at WTMLDN 2023")
 2023")










.")


 of Malaysia Tourism Promotion Board (MTPB), at Routes World 2023 in Istanbul, Türkiye.")
 at Routes World 2023 in Istanbul, Türkiye.")

 - Interview with Ulla Lettijeff, SVP and Director (Finavia), at Routes World 2023")
 New Satellite Terminal - Airports of Thailand Interview with Paweena Jariyathitipong, Senior Executive Vice President (Engineering and Construction), by Steven Howard of TravelNewsAsia.com on 15 October 2023 at Routes World 2023 in Istanbul, Turkiye.")

 - Interview with Qiang Wang, Deputy GM Aviation Business, at Routes World 2023")


 in Kazakhstan - Exclusive Video Interview with Co-Founder, Auez Tulegenov")





























")







, Hua Hin (หัวหิน), Prachuap Khiri Khan (ประจวบคีรีขันธ์), Cha-Am (ชะอำ) and Petchaburi (เพชรบุรี), to those living in Thailand as well as regional travellers and businesses.")
 has been described as 'an important enabler of Sabre’s vision for personalized travel'. But what exactly is NDC, and what role does Sabre play in its development and future growth? Those are just two of the questions that Steven Howard of TravelNewsAsia.com asks Kathy Morgan, Vice President - Offer Sourcing at Sabre Travel Solutions.")
 Conservation, Jungle Bubbles and Tourism in Thailand - Interview with John Roberts of the Golden Triangle Asian Elephant Foundation (GTAEF)")




 - State of the Industry 2020 with Subhas Menon, Director General")
, Thailand's Deputy Prime Minister and the Minister of Public Health and Dr. Tanarak Plipat, Deputy Director General of Thailand's Department of Disease Control speaking at the World Health Organisation's (WHO) COVID19 virtual press conference on 6 November 2020")









 does, as well as how the year 2019 ended and what they have planned for 2020. John tells us what Jungle Bubbles are, who is staying in them, how many elephants people can expect to see, whether they are safe, and how they plan to expand this rather unusual idea. All that and much, much more in the interview.")








 2020. Filmed at TAT's office in London on 8 January 2020, Khun Chiravadee tells us when and where TTM+ 2020 will take place, why that city was chosen, what the theme will be this year, and how many buyers and sellers are expected to attend. Khun Chiravadee tells us how many buyers from the UK will be going and how those buyers will be chosen, and much, much more.")



. Yanik tells us how the certification levels within NDC, such as Level 4 and @scale, differ from one another, why they are important, what needs to be done to go from one level to another, and so very much more.")

 in Bangkok, Steven Howard of TravelNewsAsia.com asks Robert to give us an update on the company, NDC, NGS and the industry in general.")



 Yangsuksathaporn, General Manager of the Vince Hotel Bangkok Pratunam. In this interview, filmed in the rooftop bar of the hotel on 1 November 2019, Khun Fah tells us about the location of the Vince Hotel Bangkok Pratunam, where the hotel's guests are coming from, how 2019 compares to 2018, what its USPs are, where all the creative ideas come from, which other events the hotel will attend this year, what guests can expect from the property and what plans they have for 2020. All that and much, much more in the FHD video and podcast.")








, Siem Reap (REP) and Sihanouk (KOS), how this year compares to last year, and what expansion plans they have for the future.")






, the Group Director - Travel Industry for Cape & Kantary Hotels, to ask him about the event and the company's plans for the future. In this exclusive interview, filmed at the Cape Panwa Hotel on 21 July 2019, Khun Tom tells us about three new properties the hotel group plans to open in the next few years, how they will be branded, where they will be located, and how many rooms each will have.")






 and has attended the last nine, including the most recent edition in Jomtien, Pattaya last week. In this exclusive interview, filmed on the first day of TTM+ 2019, Kati Hakkinen explains where Khanom is in Thailand, what its attraction is and what is the best way to travel there.")

 2019 in Pattaya. Steven Howard of TravelNewsAsia.com sat down with Khun Sillapat Watcharapong, Director of Marketing at the Racha Kiri Resort in Khanom, to ask him about his resort and Khanom as a destination.")

 2019, held in Jomtien, Pattaya last week, not only had the crucial buyers meet sellers component, but also different workshops with expert speakers sharing their knowledge with media and sellers alike. One such expert, Khun Arrut Navaraj, Managing Director of Suan Sampran, gave an interesting talk to delegates about Organic Farming and Sustainable Tourism.")
 in Pattaya. Mr. Tanes Petsuwan, TAT's Deputy Governor for Marketing Communications, used the media briefing to outline their plans for 2019 and beyond, and give some insight into which of Thailand's less well known destinations they will be promoting and how. This video includes the Q&A at the end.")

, in Halong, Vietnam on 26 May 2019.")






 as Miss USA. In this interview, filmed on 7 March 2019, Steven Howard asks Jazell why she has come so far to compete and why she chose Miss International Queen above all the others.")















, Managing Director of Phuket-based Sky Marine Group. In this interview, filmed at the Ocean Marina Pattaya Boat Show on 2 December 2018, Steven Howard asks Khun Thanaya about her business which includes yacht sales, hull cleaning and maintenance, as well as luxury yacht charters.")

 Song, Managing Vice President Passenger Network & Sales about the airline and its plans for the future.")

 62nd Assembly of Presidents.")


 and Sustainable Tourism - PHIST Interview. What could the World Wide Fund for Nature, or WWF as it is more commonly known, possibly have in common with the hotel industry? In this exclusive interview with Maggie Lee, Market Transformation Manager at WWF Singapore, we ask Maggie about this, and much more.")
 season and the peak November - May season.")


 forum which was held at the resort on 24 September.")







 in London.")
 at Farnborough Airshow 2018 on 16 July, Steven Howard of TravelNewsAsia.com asks Mr. Gauss about the aircraft, why it is so popular, what makes it special and what plans they have for future orders.")


















 Province, Thailand.")








